Call for Collaboration:Research on the Neural Mechanisms of Sensory Disorders and Intervention Strategies Based on the Artificial Consciousness DIKWP Model
World Academy for Artificial Consciousness (WAAC)
International Standardization Committee of Networked DIKWP for Artificial Intelligence Evaluation(DIKWP-SC)
World Artificial Consciousness CIC(WAC)
World Conference on Artificial Consciousness(WCAC)
Email: contact@waac.ac
Directory
Research Background and Scientific Questions
Research content and technical route
System diagram and pseudocode description
Key technologies and innovations
Team composition and division of responsibilities
Research Background and Scientific Questions
Perceptual impairment refers to an individual's abnormal or distorted perception of external stimuli such as vision and pain, including hallucinations, delusions, hyperesthesia or hypoesthesia. These disorders are prevalent in neuropsychiatric disorders (e.g., visual and auditory hallucinations in schizophrenia), sensory system impairment (e.g., visual hallucinations in blind patients), and chronic pain syndromes (e.g., phantom limb pain, neuropathic pain), which seriously affect the quality of life of patients. However, the mechanism of its occurrence is complex and diverse, and there is a lack of effective intervention methods. This project focuses on the two typical perceptual abnormalities of vision and pain, focusing on the national key R&D guideline "3 Analysis of the neural mechanism of perceptual impairment or abnormality and the study of new treatment strategies", and attempts to explore new intervention strategies from the multi-level integration of neural circuit mechanisms to artificial intelligence semantic models.
Typical examples of visual perception impairments include Charles Bonnet syndrome (CBS) and Alice in Wonderland syndrome (AIWS). Patients with CBS experience realistic hallucinatory images due to the absence of visual input. Studies speculate that visual hallucinations originate from retinal degeneration, causing the brain to lose normal visual inhibition, so that it autonomously activates memory images to fill the field of vision. CBS has been reported in more than 12% of patients with age-related macular degeneration (ARMD); Nearly half of people with severe vision impairment have experienced visual hallucinations. However, there is no effective treatment for such hallucinations, and previous attempts at pharmacological intervention are not ideal, and can only rely on the patient's brain to gradually adapt to reduce hallucinations. AIWS, on the other hand, is characterized by distorted perception of the size and shape of visual objects, which is thought to be associated with abnormal multisensory connections due to migraine attacks or brain infections. These phenomena reveal that visual perceptual abnormalities often stem from the mismatch between high-level semantic integration and sensory input in the brain, but the specific neural circuit mechanism still needs to be further studied.
In terms of pain perception impairment, chronic pain and phantom limb pain are typical. Chronic neuropathic pain is listed by the World Health Organization as one of the global public health priorities. According to statistics, about one-fifth of the world's population suffers from chronic pain for a long time, and a considerable part of it is neuropathic pain (such as diabetic neuralgia, postherpetic neuralgia). Phantom limb pain is an abnormality in amputees' perception that the limb is still painful when it no longer exists, and about 64% of amputees worldwide experience phantom limb pain. Studies have found that the occurrence of phantom limb pain is closely related to the spontaneous abnormal discharge of peripheral nerve stumps and the reorganization dysregulation of the central cortex. Behind chronic hyperalgesia, scientists put forward the theory of "central sensitization", that is, the pain circuits of the spinal cord and brain are plastically altered, so that the pain signal is amplified and persistent. The specific mechanisms include enhanced excitatory neurotransmission in the dorsal horn of the spinal cord (such as increased glutamate release and upregulation of NMDA receptors) and decreased inhibitory neurotransmitters (GABA, glycine, etc.), accompanied by the activation of microglia and astrocytes to release cytokines, resulting in increased neuronal excitability and pathology. At the brain level, brain imaging studies in patients with chronic pain showed abnormal functional connectivity in pain-related areas such as the somatosensory cortex, insular lobe, and anterior cingulate gyrus (ACC), and the connection between the prefrontal lobe and these areas was weakened, resulting in a decrease in the brain's ability to regulate pain and a continuous enhancement of pain experience. Existing pain treatment methods include drugs (such as opioid analgesics, antiepileptic drugs, antidepressants, etc.) and neuromodulation (such as spinal cord electrical stimulation, deep brain stimulation, transcranial magnetic stimulation). However, these therapies are often associated with significant side effects or invasive risks, and their effects are not long-lasting. For example, opioid painkillers are prone to dependence and addiction, and invasive electrical nerve stimulation carries risks such as infection and displacement, while noninvasive transcranial stimulation is short-lived and difficult to maintain in the long term. Therefore, there is an urgent need for safer and more durable new pain intervention strategies to fundamentally reshape the plasticity of abnormal pain pathways.
In summary, perceptual impairments, whether visual or nociceptive, involve multiple levels of neurological changes: from molecular and cellular (abnormalities in neurotransmitters, receptors, ion channels) to neural circuits (altered synaptic plasticity, network connection reorganization) to prediction and interpretation biases at the higher cognitive level. For example, there is growing evidence that both hallucinations and chronic pain can be explained by the "brain predictive coding" theory, in which the inconsistency of the brain's prior expectations and sensory inputs is an important cause of symptoms. When the brain is too biased towards its own "high expectations" in the internal model of the environment, it may produce hallucinatory false perceptions; Similarly, excessive expectation and attention to pain can amplify the sensation of pain. For example, studies have found that giving a positive suggestion of pain relief (placebo) significantly reduces pain sensation, while negative expectations of pain (anger effect) increase pain. In hallucination studies, the application of ketamine caused mice to develop auditory-hallucination-like illusions, and confirmed that increased dopamine release from the striatum made animals rely more on internal predictions than real inputs, thus "hearing" signals that were not there. This cross-species study of computational psychiatry showed that when modulation systems such as dopamine in the brain are out of balance, the weight of high-level intention/expectation over perception is too high, which can lead to abnormal perception. This finding provides a new circuit perspective for understanding hallucinations and perceptual abnormalities, and suggests that it is possible to intervene in such symptoms by modulating the processing of purpose/desired information in the brain.
Based on the above background, this project realized that in order to solve perceptual barriers, it is necessary to adopt a new multidisciplinary approach: on the one hand, it is necessary to deeply analyze the neurobiological mechanism, and on the other hand, introduce artificial consciousness models in artificial intelligence for cross-level modeling, and carry out unified description and intervention from the data layer (sensory signals) to the knowledge layer and the purpose layer (high-level cognition). Relying on the advantages of the disciplinary platform of the Active Medicine Committee of the World Association of Artificial Consciousness, this project intends to use the DIKWP artificial consciousness model (Data-Information-Knowledge-Wisdom-Purpose) as a theoretical framework to combine biological neural mechanisms with artificial intelligence semantic cognition models to answer the following scientific questions:
What are the neurogenesis mechanisms of perceptual impairment (represented by visual hallucinations and chronic pain) at the molecular, cellular, neural circuit, and systemic behavioral levels? How do the different levels of mechanisms interact to lead to the creation and maintenance of anomalous perception?
What are the existing interventions for perceptual abnormalities (drugs, neuromodulation, psychotherapy, etc.) on the nervous system? What is the underlying cause of its limited efficacy? How can new theoretical models guide improvement strategies?
How can the DIKWP model of artificial consciousness be used to simulate the human perception process and decompose the brain's processing of perceptual information into five layers: data-information-knowledge-wisdom-purpose? Can the model be used to build a mechanism of "anomaly recognition" and "semantic reasoning" to understand and detect anomalies from the perspective of artificial intelligence?
Based on the cognitive architecture of the artificial consciousness model, how to design a digital simulation platform to realize the simulation experiment of perceptual impairment and intervention programs without the need for physical experimental equipment? What core modules (such as perceptual semantic interfaces, cognitive reconstruction engines, feedback modulation channels, etc.) are required for such a platform to operate in a closed loop?
Are there new interventions, such as semantic-driven cognitive restructuring or artificial consciousness-guided adaptive neuromodulation, that can break through the limitations of traditional drug/electrical stimulation therapies? Can the effectiveness and innovation of these new strategies be demonstrated through simulation and the necessary validation of animal behavior?
Focusing on the above problems, this project aims to propose a new research paradigm for perceptual impairment: multi-level integration research based on brain science experimental data and artificial consciousness model, so as to provide a new way to elucidate the mechanism of perceptual abnormalities and innovate therapies. This is not only of great theoretical significance (it is expected to break through the existing one-sided understanding of hallucinations and pain mechanisms), but also has potential clinical applications and industrial transformation prospects (such as the development of digital therapeutics, intelligent assisted diagnosis and treatment systems), and sets a model for the intersection of artificial intelligence and neuroscience. In particular, it is worth emphasizing that although this project lacks the foundation of large-scale physical experimental equipment, it is expected to achieve a breakthrough in the form of "corner overtaking" based on solid theoretical and model innovation, and make a leading voice in international academic dialogue.
Research Objectives:
The overall goal of this project is to elucidate the neural mechanisms of visual and pain perception disorders and develop innovative intervention strategies based on artificial consciousness using the DIKWP model of artificial consciousness. The specific objectives are as follows:
Multi-level neural mechanism analysis: Using the research results of molecular biology, neuroelectrophysiology, brain imaging and behavior, this paper systematically elucidates the mechanism of visual hallucinations and chronic pain abnormalities from peripheral receptors to central nervous networks, and reveals key targets and circuit changes. He focuses on mechanisms such as synaptic plasticity changes, glial cell-mediated neuroinflammation, brain interval connection recombination, and brain prediction error processing.
Analysis of the Mechanism and Limitations of Existing Therapies: This paper summarizes the principles of action of current drugs (such as dopamine antagonists, opioids), physical stimulation (such as transcranial magnetism, spinal cord electrical stimulation) and psychological/behavioral therapies in correcting perceptual abnormalities, and analyzes their shortcomings in combination with mechanism studies. For example, why can't medication eliminate CBS hallucinations? Why is neuromodulation difficult to provide long-lasting relief of chronic pain? The DIKWP model was used to model the semantic logic of these intervention pathways, and the key links that were not touched by traditional therapies were extracted.
DIKWP Artificial Consciousness Model Application: Build a DIKWP model implementation specifically for perceptual abnormalities, including: anomaly perception recognition module (detecting abnormal patterns output by each layer of DIKWP, such as wrong "information" or distorted "Wisdom" layer decision-making), cross-brain region semantic reasoning algorithm (simulating the role of different brain regions in knowledge and wisdom layers of semantic interaction, reconstructing the multi-region consistency required for normal perception), and an artificial consciousness operating system (OS) framework that integrates the above modules. Under this framework, the autonomous perception, self-reflection and abnormal alertness of the artificial intelligence system to external stimuli are realized, and the process of screening and correcting perceptual information by human consciousness is simulated.
Artificial Intervention Strategy and Digital Simulation Platform: Develop an interactive digital simulation platform to conduct in silico experiments on perceptual abnormalities and their interventions by using the constructed artificial consciousness OS and perceptual semantic model. The platform includes a perceptual semantic interface (which converts sensory signals in a real or simulated environment into the data layer input of the DIKWP model, and can introduce noise or anomalies to simulate pathological conditions), a cognitive reconstruction engine (dynamically adjusts the parameters or structures of each layer of the model according to the type of abnormality detected, which is equivalent to imposing interventions, such as reducing the weight of error priors, simulating drugs to block a pathway, etc.), and intervention feedback channels(Monitor the "Wisdom" layer results of the simulation output, i.e., the final perceived experience, evaluate the effect of the intervention and guide the next adjustment). Through repeated iterations of the platform, the optimal combination of intervention strategies was screened.
Validation and Evaluation of Innovative Therapies: 2-3 innovative intervention strategies for perceptual abnormalities are proposed on digital platforms, such as semantic-guided neurofeedback therapy (real-time reminder and correction of patients' unreasonable perceptual interpretations through artificial consciousness systems to reduce hallucinations/pain) or lead drugs (designed for newly discovered molecular targets and tested in simulation). The scheme with outstanding effect was selected and initially verified on the animal behavior model (e.g., a mouse model with a VR visual hallucination environment was constructed to test the deviation correction effect of the semantic interface; or use pain model mice to test the effects of the new drug on pain behavior and neural activity). Evaluate the effectiveness, stability, and innovation of these strategies to lay the foundation for further clinical translation.
Through the achievement of the above objectives, this project is expected to produce a new theoretical model of perceptual impairment, reveal several key mechanisms and propose original intervention pathways. On this basis, a set of systematic methods for AI-assisted perception of abnormal diagnosis and treatment will be formed, which will provide technical reserves for the future development of digital medical products (such as hallucination management assistance system, pain cognitive intervention APP, etc.).
Research content and technical route
In order to achieve the research objectives, the project has designed four interconnected research content modules, each of which corresponds to a specific technical route and methodology. The research content and technical route are shown in Figure 1:
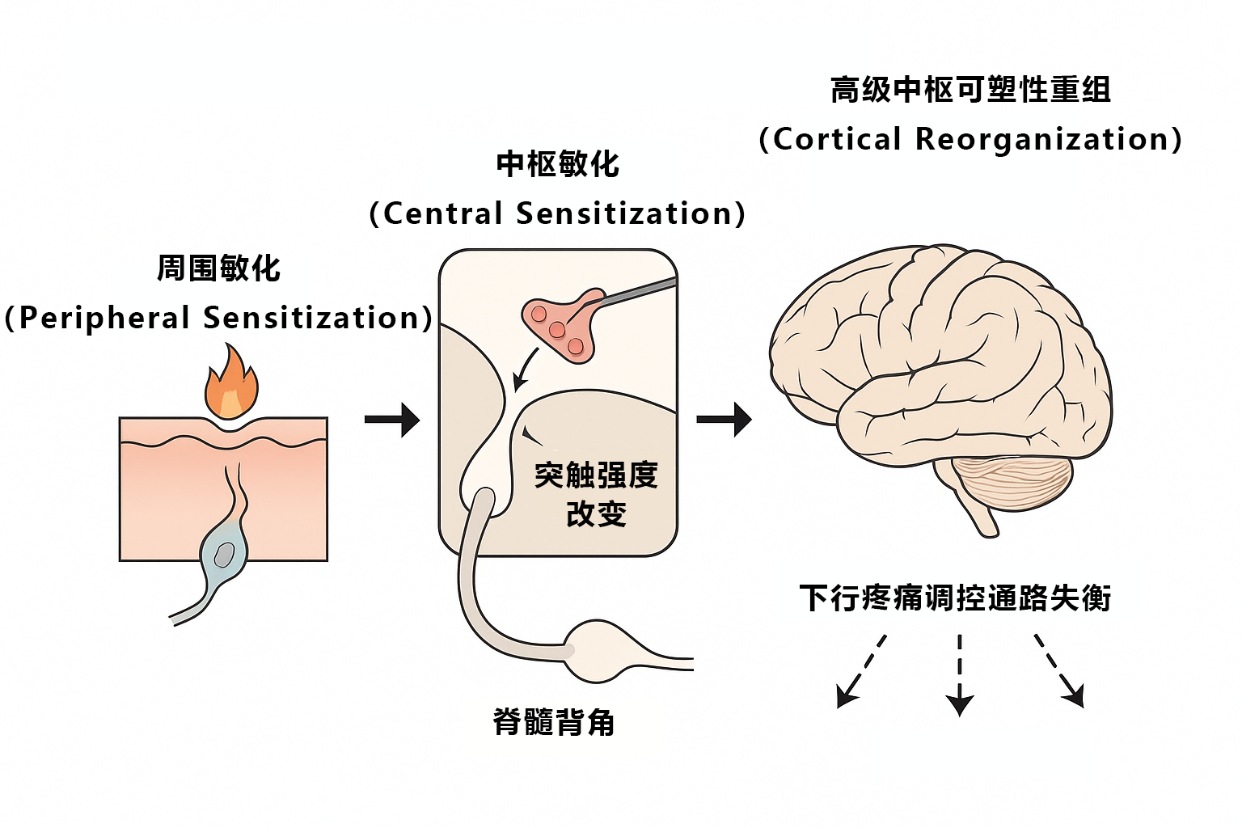
Figure 1: Illustration of the multi-level mechanisms by which pain perception disorders occur. The figure shows the whole process of chronic pain from peripheral inflammation-mediated peripheral sensitization, to central sensitization due to synaptic plasticity changes in the dorsal horn of the spinal cord, to the reorganization of cerebral higher-level central plasticity and the imbalance of descending pain regulatory pathways. Together, these multi-layered mechanisms shape the occurrence of chronic algesia. This project will systematically investigate visual hallucinations and hyperalgesia for similar multi-level mechanisms.
1. Research on the neural circuit mechanism of perceptual impairment: Firstly, an in-depth literature survey and data analysis were carried out to sort out the neurobiological mechanism basis of visual and pain abnormalities. Through the review of relevant research in recent years, the important findings are extracted. For example, visual hallucinations focus on how spontaneous activity of the visual cortex produces visual hallucinations, the role of visual associations such as the preparietal area in hallucinations, and the influence of neurotransmitters such as 5-HT and Ach systems in visual abnormalities. In terms of pain dysphoria, the focus is on changes in the dorsal horn neural circuit of the spinal cord in pain amplification (e.g., dysregulation of excitability/inhibition), decreased modulation of pain sensation by the descending pathway of the brainstem PAG-bulbar RVM, and limbic system(such as the amygdala) role in the amplification of chronic pain, etc. If possible, we will work with relevant laboratories to obtain some experimental data, such as changes in brain networks for visual hallucinations revealed by functional magnetic resonance imaging (fMRI) and changes in neural electrical activity recorded in animal models of pain. By integrating multi-level evidence, the "mechanism map of visual hallucinations" and the "mechanism map of chronic pain abnormalities" were drawn to clarify the key molecular-cell-circuit links and interrelationships involved in each abnormality**. As shown in Figure 1, we connected the abnormal transmission of nerve impulses caused by peripheral neuropathy, the changes in spinal cord and brainstem plasticity, and the reconstruction of brain plasticity into a network to find the nodes that are most worthy of intervention.**
On this basis, we apply computational modeling methods to verify some mechanisms. For example, a dynamical model can be used to simulate how increased excitability gain in a neuronal network triggers spontaneous activity (corresponding to hallucination), or a Bayesian brain model can be used to simulate how the brain perceives pain by combining a priori and evidence. These models validate the plausibility of our mechanism hypothesis, and support the hypothesis if the simulation results are consistent with the real anomaly. If the differences are significant, the understanding needs to be adjusted.
2. Mechanism of action and limitations of existing treatments: This content aims to answer: Why are current treatments insufficient? How to find improvement ideas in combination with mechanism research. We will classify the main treatment modalities for hallucinations and chronic pain, and analyze their sites of action at the neural circuit level
Medications: For visual hallucinations, such as schizophrenia, antipsychotics (dopamine D2 receptor antagonists) are often used to reduce dopamine overactivity, but have no obvious effect on hallucinations caused by pure sensory loss (such as CBS); For chronic pain, typical drugs include NSAIDs (peripheral anti-inflammatory analgesics), opioids (central pain threshold increases), and anticonvulsants such as gabapentin (which reduce neuronal excitability). By reviewing pharmacological and clinical data, we will summarize the mechanisms and shortcomings of these drugs, such as long-term opioid use can trigger tolerance and addiction, and antipsychotics have limited efficacy and large side effects on visual hallucinations. Combined with the mechanism map, we analyze the links covered and the gaps that are not covered by the drug's action. For example, opioids act primarily on central μ receptors to inhibit pain signaling, but do not reverse changes in the plasticity of central sensitization, so pain may recur after discontinuation of the drug. We try to simulate drug effects using the "data-information" layer of the DIKWP model: think of the drug as an increase or decrease in nerve signals (data flow) or noise suppression, such as opioids that reduce the intensity of the "pain data" stream, dopamine antagonists that reduce the weight of false "predictions", etc. Through this semantic modeling, it is clear that the drug can only temporarily modulate the data**/information layer, and the** abnormal cognition** of the knowledge/wisdom layer is not corrected, which may be the reason for the easy rebound of efficacy.
Neuromodulation techniques: including invasive spinal cord stimulation (SCS), deep brain stimulation (DBS), and non-invasive transcranial magnetic stimulation (rTMS), transcranial direct current stimulation (tDCS), etc. The common principle of these techniques is to directly modulate the excitability of specific neural circuits, such as SCS by transmitting array stimulation in the dorsal column of the spinal cord, activating local inhibition of intermediate neurons, thereby "shutting down" pain conduction; DBS administers high-frequency electrical stimulation to the thalamus or limbic system, interrupting abnormal signaling circuits; rTMS/tDCS can non-invasively alter cortical excitability. We will investigate the progress and limitations of the use of these methods in hallucinations/pain. For example, transcranial magnetic stimulation to inhibit the visual cortex to alleviate visual hallucinations has been tried in the field of visual hallucinations, but efficacy has been inconsistent; In the field of pain, rTMS stimulates the motor cortex to have a certain analgesic effect, but the effect is short-lived. Using the DIKWP model, we see neuromodulation as an external calibration of the "information-knowledge" layer: for example, transcranial magnetism directly changes the processing threshold of information in a certain area of the brain (e.g., reducing the production of visual cortex noise), and DBS is equivalent to a high-frequency interference of abnormal knowledge connections in the circuit, causing them to temporarily fail. However, we speculate that this type of physical means is not sustainable because the brain's purpose/destination layer drive** gradually adapts the network to external stimuli (i.e., there is tolerance or plastic rebound), so the anomaly may return after the stimulation is stopped.
Psychological and behavioral therapy: including cognitive behavioral therapy (CBT), attentional bias training, mirror therapy, etc. For example, people with phantom limb pain often use mirror therapy to "see" the missing limb and move it to relieve pain with the help of visual feedback. This is actually an intervention that uses visual semantics to correct pain cognition, recalibrating the brain's knowledge and purpose of pain. CBT also has some effect on patients with chronic pain and hallucinations, by guiding patients to change their cognitive and emotional responses to symptoms (i.e., adjusting the interpretation and value judgment of perception in the "Wisdom" layer). We will collect research data from these therapies and analyze their active ingredients. For example, mirror therapy is thought to reduce the false body image reorganization associated with phantom limb pain and restore normal connections in some parts of the sensory-motor cortex; CBT may enhance inhibition of downstream nociception/hallucination signals through the prefrontal-limbic pathway. The DIKWP model is used to interpret the behavioral**/psychological intervention directly on the knowledge-wisdom-purpose layer**, changing the interpretation framework and goal orientation of the input data of the AI system, thereby affecting the perceptual experience of the output. The advantage of this type of therapy is that it targets high-level mechanisms and therefore may lead to more lasting improvements (because it changes the "software" rather than just intervening in the "hardware" signal). However, its limitations are that the effect is slow, individual differences are large, and it requires the subjective cooperation of patients.
Through the above analysis, we will identify key links that have not yet been covered by conventional therapies. For example, if neither drugs nor physical stimulation are found to be able to restore the brain's normal interpretation of sensory signals (see Wisdom Layer Problem), then new therapies should focus on this. Conversely, if some molecular pathways (data layer issues) cannot be specifically regulated by existing means, we will also consider the development of corresponding new drugs. The output of this part of the research will be a "mechanism-limitation" analysis report and a corresponding description of the DIKWP semantic model for each of the existing therapies, which will provide direction for innovative strategies.
3. Abnormal Perception Recognition and Semantic Inference of the Artificial Consciousness DIKWP Model: After mastering the biological mechanism and the traditional therapeutic landscape, the core innovation of this project lies in the introduction of the DIKWP artificial consciousness model to simulate and understand the human perception process, and to design anomaly detection and semantic inference algorithms accordingly. The DIKWP model is composed of five layers: Data, Information, Knowledge, Wisdom and Purpose, which is an informatics depiction of human cognition/consciousness processes. Applied to the field of perception, it can be explained as follows:
Data layer: Raw signal input from a sensory organ, equivalent to an unprocessed nerve discharge or pixel stimulus. For vision, it is a light stimulation signal for the retina, and for pain perception, it is an electrical signal for nociceptors.
Information layer: Characterization of data after initial processing and feature extraction. For example, the edge and shape of the vision, or the intensity and location of the painful stimulus. Biologically corresponds to a low-level sensory center (limbic detection of visual cortex V1, spinal/thalamic coding of pain intensity). This step turns cluttered data into meaningful schema information.
Knowledge layer: Synthesize multimodal information and combine memory and learning to form an understanding of the current situation. Visually, it's the process of identifying "what you're seeing is a cat"; In terms of pain, it is to know that "the pinprick sensation of the hand means injury". The knowledge layer involves the invocation of past experience and semantic memory. In the brain, this corresponds to a wide range of junction areas and hippocampal/neocortex synergy.
Wisdom Layer: Builds on knowledge to make higher-level judgments and decisions, including situational understanding, value evaluation, and strategy selection. For example, being aware that "this is just a hallucination, not real" or "persistent back pain may mean a serious cause that requires medical attention." The Wisdom layer introduces values and long-term experiences to connect perceptions with behavioral decisions.
Purpose Layer: The flow of information that runs through and drives the above levels, representing the goals, motivations, and concerns of the system. Purpose determines where to focus attention and what to expect from perception. For example, a strong desire to see something can affect visual processing tendencies, and a person who is afraid of pain may have an overawakened layer of the brain that amplifies pain signals. Purpose is the core driving force of the model, ensuring that the processing of each layer is directional.
In the context of DIKWP, perceptual impairment can be seen as a result of deviations in processing at all levels. For example, hallucinations can be interpreted as the fact that the information layer noise is misidentified as a real signal by the knowledge layer, and the Wisdom layer fails to properly label its false nature; Chronic hyperalgesia can be seen as a weak signal in the data layer that is given too high a threat weight through the knowledge layer, and the Wisdom layer makes an excessive pain response decision. In response to this understanding, we will develop the following key modules in the Artificial Consciousness OS:
Anomaly Perception Recognition Module: Listens to the status of each layer of the DIKWP model when processing external inputs, and triggers an alarm once an abnormal pattern occurs. In terms of specific implementation, a set of monitoring indicators can be designed for the model, such as a sudden increase in the output entropy of the information layer (indicating the possibility of hallucinatory noise), a large difference between the output of the knowledge layer and the historical norm, and an abnormally low or high decision-making confidence in the Wisdom layer. Once the indicator crosses the bounds, it is judged that there is a perceptual anomaly. This module is similar to the "self-monitor" of artificial consciousness, allowing AI to supervise its own perception process. For example, when a pattern is "seen" that is not real, the information-knowledge match of the model decreases, and this disagreement can be used as a warning sign for hallucinations. As another example, pain can also be considered abnormal if the Wisdom level decision (pain response intensity) is significantly inconsistent with the objective stimulus. We will use existing anomaly detection algorithms (such as Bayesian prediction error-based detection) combined with the DIKWP hierarchy for custom development.
Semantic reasoning algorithms across brain regions: When the human brain processes perceptual information, multiple brain regions often cooperate to form a "global workspace" or semantic network. This inspires us to introduce cross-module semantic inference in the DIKWP model: that is, in the knowledge and wisdom layer, multiple semantic nodes are introduced to represent the knowledge of different brain regions, and each node transmits information to each other through the graph network or Transformer architecture to jointly reason the meaning of perception. For example, in the case of visual hallucinations, the output of the visual cortex node contradicts the information of the cognitive node of the prefrontal lobe (the prefrontal lobe may have experience knowing that something should not appear in this situation), and the error of the visual node can be corrected through semantic exchange. In terms of implementation, we will adopt the method of graph neural network (GNN) or multi-agent collaborative inference: each agent represents a functional brain region, has a local knowledge base and inference rules, and coordinates through message passing. The algorithm needs to solve the problems of heterogeneous information fusion, conflict detection and consistency convergence, and can learn from AI inference models such as blackboard model or Bayesian network. In the case of pain, such an algorithm can combine somatic sensory information with emotional background and memory information to determine whether the pain signal is reasonable. For example, when reasoning across brain regions leads to "no harm at the moment but still a strong pain signal", abnormal amplification can be assumed to be present, which triggers intervention recommendations.
AC Operating System: The functions of each layer of the DIKWP model, anomaly detection and semantic inference modules are integrated into a single operating environment to realize the unified scheduling of data flow and the interface of human-computer interaction. This is similar to equipping an artificial consciousness model with a "conscious brain". The OS will be responsible for receiving input from the simulated environment (the data layer feeds the model sensory interface), managing the processing threads at each layer, generating action decisions or feedback outputs to the environment at the Wisdom layer, and presenting the internal state of the model on the HMI (e.g., visualizing the semantic content of each layer). The operating system also needs to include a metacognitive loop, a cycle in which the model evaluates and adjusts its own state. Professor Yucong Duan proposed the DIKWP × DIKWP dual-cycle architecture, which can be introduced as a reference. We will try to implement a metacognitive agent that responds to the output of the anomaly perception recognition module, adjusting the model parameters as needed (e.g., reducing some bias in the Purpose layer). The final OS should enable the artificial consciousness model to achieve a closed loop from perception, cognition to action in the simulated environment, allowing us to observe and intervene in the model's perceptual anomalies through the platform.
The development of the above modules will use programming languages such as Python or C++, using deep learning frameworks to build the necessary neural network models, supplemented by symbolic AI methods to implement inference mechanisms. The AI engineers in our team will write the corresponding algorithm code and conduct unit tests and integration tests. Pseudocode 1 shows the basic idea of anomaly detection and intervention algorithms:
# Pseudocode 1: Anomaly Perception Detection and Intervention Process in Artificial Consciousness OS
initialize DIKWP_model # Initialize the parameters of each layer of the artificial consciousness model
loop:
sensory_data = get_environment_input() # Get environmental sensory input
info = DIKWP_model.data_to_info(sensory_data) # data-> information processing
knowledge_repr = DIKWP_model.info_to_knowledge(info) # information - > knowledge
wisdom_decision = DIKWP_model.knowledge_to_wisdom(knowledge_repr) # knowledge-> wisdom decision
output_action = DIKWP_model.wisdom_to_action(wisdom_decision) # Generate actions/feedback based on the Wisdom layer output
# Anomaly perception and identification
if detect_anomaly(info, knowledge_repr, wisdom_decision):
anomaly_type = classify_anomaly_pattern(info, knowledge_repr, wisdom_decision)
log("Anomaly detected: " + anomaly_type)
# Collaborative correction of semantic reasoning across brain regions
adjusted_knowledge = cross_region_semantic_inference(knowledge_repr, context_memory)
revised_decision = DIKWP_model.knowledge_to_wisdom(adjusted_knowledge)
# Trigger intervention
if anomaly_type == "Hallucination":
# For example, reduce the weight of visual information to enhance the rational judgment of the prefrontal lobe
DIKWP_model.adjust_layer_parameter(layer="info", param="gain", value=lower)
elif anomaly_type == "hyperalgesia":
# For example, reduce the prior intensity of pain and increase the pain suppression signal
DIKWP_model.adjust_layer_parameter(layer=" Purpose ", param="pain_expectation", value=reduce)
continue # Restart the next cycle (let the model re-perceive after adjustment)
endif
perform_action (output_action) # Perform model output (e.g., produce a reaction to the environment or provide user feedback)
end loop
Pseudocode 1 describes the general cyclic flow of an artificially conscious operating system. When a perceptual anomaly is detected, the system first adjusts the internal representation through cross-region semantic inference, and then modifies the model parameters according to the anomaly type (equivalent to taking interventions) before entering the next perceptual cycle. This enables a closed-loop control: continuous monitoring, identification of anomalies, intervention, and re-observation.
4. Design of perceptual abnormality intervention strategy and construction of digital simulation platform: After obtaining the artificial consciousness OS, we will enter the application stage of research, with the goal of building a digital simulation platform for testing the effects of various intervention strategies on perceptual abnormality. The platform consists of the following components:
Virtual Environment & Sensation Interface: Create customizable, simulated environments to present visual and pain-related scenarios. The visual environment can use Unity3D or VR technology to generate realistic 3D scenes and stimuli that may induce hallucinations (such as random flashing light and shadow in low-light conditions, and the guidance model may be misjudged); The pain environment simulates a virtual organism with a "pain sensor" through a computer model, or directly builds a mathematical function to generate pain signal inputs (which can be fitted based on real pain neuronal firing data). The artificial consciousness OS obtains these environmental signals through the perception interface to achieve "virtual perception". The interface needs to support the introduction of noise or anomalies, such as we can overlay random patterns on the visual data to simulate visual triggers, and continuous background discharges on the pain data to simulate neuropathic pain. The interface will also record the model's behavioral responses to the environment (e.g., the model "reports" what it sees, or exhibits pain-avoiding actions) for us to evaluate the effect of the intervention.
Intervention Strategy Library: We will implement a variety of controllable intervention methods in the platform for flexible combination testing. These include: 1) Virtual drug: Insert an operation to change parameters in a certain layer of the model to simulate the effect of the drug. For example, the "blocker" is set to act on the data-> information conversion function to reduce the signal intensity by a certain percentage (similar to the effect of anesthetic); or act on a certain type of signaling pathway at the knowledge layer, increasing its threshold (similar to antipsychotic inhibition of over-predictive signals). 2) Virtual electrical stimulation: The output of a node inside the model is regularly forced to modify to simulate the intervention of electrical stimulation. For example, the abnormal peaks in the pain information flow are cut each cycle, or the visual information buffer is reset periodically, simulating the intervention of TMS in the visual cortex. This can be achieved by including trigger conditions in the loop. 3) Semantic correction: The feedback channel of the artificial consciousness model itself is used to apply high-level information to the low-level to achieve "cognitive regulation of feelings". For example, when an illusion is detected, the Wisdom layer outputs a signal to the information layer, prompting that it may be an illusion, and the information layer reduces the credibility of the corresponding signal. This is similar to the process by which the patient informs himself that his hallucination is unreal through volitional awareness. We can also design an external intelligent agent to act as a "therapist" that reads the model state and sends semantic guidance. 4) Novel strategies: including the semantic-driven refactoring and lead drugs we conceived. Semantic-driven refactoring refers to influencing perception by modifying the model's Purpose layer without relying on external physical actions (e.g., dynamically adjusting the model's attention allocation so that it no longer focuses excessively on anomalous stimuli); The lead drug is based on mechanism discovery, and tests drugs with new targets in simulation, such as blocking glial cell-mediated inflammatory pathways, to see if it can reduce abnormal pain signals. These strategies can enable complex interventions through combinations, such as the "drug + semantics" combination: reducing the underlying signal intensity and altering the top-level cognitive evaluation at the same time may be more effective than a single measure.
Evaluation & Feedback Module: In order to objectively measure the effectiveness of the intervention, we pre-set a series of evaluation indicators. For example, "hallucination rate" (the number of hallucinations reported by the model per unit time), "pain score" (the numerical value of pain intensity output by the model's Wisdom layer), etc. The platform will automatically record the curves of these indicators under different intervention strategies. We will use commonly used statistical tests to compare whether the effects of different strategies are significantly better than no intervention or the current standard intervention. For example, a strategy is considered to have potential if it reduces the incidence of hallucinations by more than 80% and has fewer side effects (interference with normal perception). The feedback module is also linked to the anomaly detection module to continuously monitor new anomalies as the intervention is in progress, and dynamically adjust the intervention parameters when necessary to achieve closed-loop optimization. For example, if the model shows signs of tolerance to an intervention (metrics begin to pick up), the system can prompt an increase in the dose or the addition of an adjunctive strategy.
The digital simulation platform will be presented with a user-friendly interface, allowing researchers to easily configure experiments. For example, select the intervention combination through the drop-down menu, set up a simulation scenario (such as "no one room at night" to induce visual hallucinations, "continuous inflammatory input" to induce pain abnormalities), and see the state changes and output behaviors of the DIKWP layer inside the model in real time after running. This is the equivalent of a "digital lab" capable of repeatingly, multifactorily testing hypotheses without the need to consume real lab animals or endanger patients. Considering that there is no physical equipment foundation for this project, the construction of this platform is an important guarantee to ensure the execution of research tasks, and it is also a reflection of the innovation of the project. It allows us to iteratively screen out the best solutions in a cost-effective and efficient manner, and then devote limited resources to biovalidation of the most promising strategies.
5. Animal simulation verification and pilot mechanism exploration: In order to improve the credibility of the research conclusions, we plan to select key findings for preliminary reality verification in the later stage of the project, mainly by simulating and intervening in the corresponding perceptual abnormalities on animal models. Due to the lack of large-scale experimental instruments in this project, we will use the support of cooperative units or public data resources for verification, and the specific solutions include:
Animal Behavior Simulation of Visual Hallucinations: Mice were selected as models to reflect visual perception using their avoidance behaviors. For example, we can build a simple maze in which a certain section of the path wall is projected with dynamic light and shadow interference, and mice may exhibit confusion or misjudgment of the path (similar to hallucinatory illusions). Our intervention was to reduce the number of misbehaviors in mice by presenting cue signals on a micromonitor carried by mice (corresponding to semantic interventions) or by optogenetic means to inhibit specific neuronal activity in the visual cortex (corresponding to physical interventions). If we are unable to conduct experiments in person, we can also use the literature to find out if there are similar experimental results, such as reports that inhibiting the activity of the anterior visual patrimbulum area of mice can reduce their optical illusion behavior, etc., as a validation support.
Animal model validation of chronic pain: Classical pain model mice (e.g., chronic sciatic nerve ligation model, elicit neuropathic pain) were employed. Behavioral (e.g., mechanical foot reflex threshold) and fiber-optic in vivo imaging techniques were used to evaluate the feasibility of our proposed intervention ideas. For example, we predicted that a drug targeting glial cells would attenuate central sensitization, so we gave an experimental glial inhibitor to the experimental group of mice, when available, to record changes in pain behavior. Or use the brain-computer interface method to train mice with real-time neurofeedback: when excessive activity in their pain-related brain regions (ACC, etc.) is detected, the reward pathway is stimulated to inhibit the activity, so as to achieve analgesia (corresponding to semantic-driven intervention ideas). The success of these attempts will provide valuable information for our model: success proves that the model is correct, and failure can be analyzed to feed back the model improvement.
Key Mechanism Biological Indicator Detection: Based on simulation and model analysis, we may propose new biological indicator predictions. For example, if our model shows that hallucinatory tendencies are closely related to striatal dopamine levels, we can use mouse behavioral experiments combined with microdialysis to measure the amount of striatal DA released when hallucination-like behaviors are induced to verify the association. If it can be confirmed that dopamine-driven high prediction weights lead to hallucinations, the influence of this project theory will be greatly enhanced. Similarly, for pain, we may focus on inflammatory factor levels, synaptic plasticity markers (e.g., pERK expression in the dorsal horn of the spinal cord), etc., and collaborate to obtain such data to support our inferences.
Through the above-mentioned multi-level and multi-method research content design, we will gradually realize the closed-loop research from basic mechanism understanding to model construction, to strategy development and validation. The innovation in the technical route lies in the fact that artificial intelligence models and digital simulation methods are fully used to replace some traditional experiments, which not only reduces costs, but also enables us to explore more hypotheses; At the same time, the key bioverification link is retained to ensure that the conclusions are not disconnected from reality. This technical route of "virtual and real combination" is very much in line with the current development trend of scientific research (such as the application of digital twins in medical treatment), and also provides a feasible path for this project to produce high-quality results without large-scale experimental instruments.
Three-year task breakdown
The planned implementation period of this project is three years (36 months), and the phased tasks are divided according to the research content and technical route, which are broken down as follows:
Year 1 (0-12 months): Theoretical research and model design stage.
*Task 1: Literature research and mechanism review (0-6 months). *In the past 10 years, we will review the research papers and reviews on visual hallucinations and phantom limb pain/chronic pain at home and abroad, and sort out important molecular, cellular, circuit mechanisms and treatment progress. Interdisciplinary seminars were held 1-2 times, and experts in neurobiology and clinical medicine were invited to discuss mechanistic hypotheses. Output: A review of the neural mechanisms of abnormal visual perception and a review of the neural mechanisms of abnormal pain perception each report, as well as the corresponding indication Purpose.
*Task 2: Preliminary design of the DIKWP model (3-9 months). *Led by the artificial intelligence sub-research group, the elements of the perception process obtained from the investigation were mapped to the DIKWP framework to form a model sketch. Write the prototype code of model simulation to realize the basic data-information-knowledge flow. The model's perceptual behavior of simple stimuli under normal conditions was tested in a simulated environment, and the parameters were adjusted to ensure that the model output was reasonable when there was no abnormality. At the end of the first year, the DIKWP Perception Model Technical White Paper and model code V1.0 were submitted.
*Task 3: Semantic analysis of existing therapies (6-12 months). *Medicine collaborates with AI personnel to perform semantic logic modeling of commonly used therapies. The effects of 1-2 typical therapies (e.g., analgesics, anti-hallucinogenic drugs) were simulated in the DIKWP model to observe the behavior changes of the model. Comparative analysis reports are formed to identify deficiencies in existing interventions. Prepare for the first mid-term review meeting of the project and present the results of the phase.
Year 2 (13-24 months): Model implementation and platform development phase.
*Task 4: Artificial Awareness OS and Anomaly Detection Module Development (13-18 months) *Improve the algorithms of each layer of the DIKWP model to achieve real-time anomaly detection. It focuses on overcoming cross-brain semantic reasoning algorithms to optimize their efficiency and accuracy. In the simulation, abnormal inputs are artificially created to verify whether the detection module can be captured in time. Output: "Technical Report on Anomaly Recognition Algorithm", and applied for 1 software copyright ("Artificial Awareness Monitoring System for Perceiving Anomalies V1.0").
*Task 5: Digital simulation platform construction (16-22 months). *Engineers and technicians build a user-friendly interface to connect the model to the virtual environment. Development of intervention strategy library functional modules. Internally test the impact of different intervention combinations on the model and debug the stability of the platform. By the end of the second year, the platform V1.0 will be completed, and basic simulation experiments can be carried out.
*Task 6: Preliminary simulation experiments and strategy screening (20-24 months). *Run multiple sets of simulation experiments: for example, set up a visual hallucination scene, and run the model 10 times each with no intervention and different interventions to compare the frequency of hallucinations; Set up abnormal pain scenarios and compare the "pain scores" of the models under each strategy. Use statistical analysis to identify 2-3 combinations of strategies that perform best. The "Evaluation Report on the Effect of Simulation Intervention" was formed. The second project meeting was held, and domain experts were invited to review the platform and model results to provide suggestions for the next step of animal validation.
Year 3 (25-36 months): Strategy validation and refinement phase.
*Task 7: Animal simulation validation (25-30 months). *In conjunction with partner laboratories, animal experiments were validated for key strategies for screening in the second year. Acquire and analyze behavioral data or biomarker data. At the same time, the simulation model is improved, and the parameters are adjusted according to the experimental results (for example, if it is found that the effect of a certain strategy is weaker than the simulation prediction on animals, the model is modified after analyzing the reasons). Completed the "Report on the Preliminary Results of Animal Experiments".
*Task 8: Model optimization and training (28-34 months). *Based on the simulation and experimental evidence, the DIKWP model was finally optimized. This includes improving the parameter learning mechanism of the Purpose layer, improving the robustness of anomaly detection, and increasing the adaptability of the model to diverse scenarios. Finally, the model architecture was frozen, and a complete intervention system for artificial consciousness perception abnormalities was established. Preparation of relevant patent application documents (2 patents are expected: one on "Perceptual Anomaly Detection Method Based on Artificial Consciousness" and one on "Digital Simulation Intervention System for Perceptual Anomaly").
*Task 9: Summary of results and application outlook (31-36 months). *Write research papers and project reports summarizing findings and innovations over the past three years. It is planned to write no less than 3 high-level papers (target journals such as Neural Networks, Frontiers in Neuroscience, Science China, etc., including at least 1 English SCI paper), covering mechanism research, model methods, simulation platforms and results. Hold a project results conference to demonstrate the platform to the World Artificial Awareness Association and peers in the field of medical AI, and strive for further cooperation or transformation opportunities. Prepare the project acceptance materials, including technical reports, paper patent lists, final account reports, etc., to ensure the successful conclusion of the project.
The above-mentioned task schedule will be appropriately adjusted according to the actual progress, but in general, it will ensure that there are phased results every year: the first year will consolidate the theoretical and model foundation, the second year will achieve core technology breakthroughs and provide simulation results, and the third year will verify and improve and produce landmark results. In terms of project management, the project leader organizes progress discussions every quarter, coordinates resources and adjusts plans in a timely manner, and ensures that all tasks are completed on time and with quality.
System diagram and pseudocode description
During the implementation of this project, several key system architecture diagrams and algorithmic pseudocode were generated to illustrate the concept and technical implementation. In this section, we will excerpt some of them for explanation.
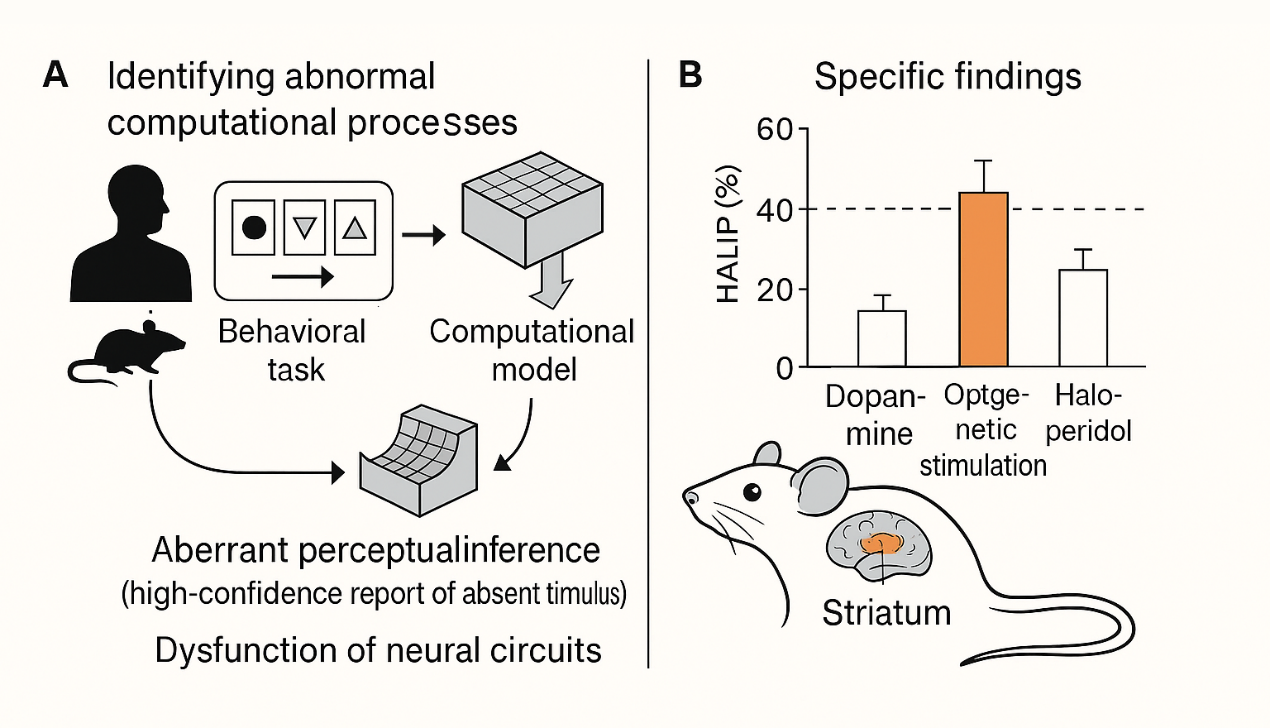
Figure 2: A cross-species computational psychiatric approach reveals the neural circuit mechanisms of hallucinations. Figure A (left) illustrates the design of behavioral tasks and computational models to find anomalous computational processes that elicit hallucination-like perceptions in humans and mice. The results suggest that abnormal perceptual reasoning (reporting non-existent stimuli with high confidence) stems from dysfunction of neural circuits. Panel B (right) shows the specific findings: when mice with elevated striatal dopamine levels, the incidence of high-confidence false reporting (HALIP) was significantly increased; Using optogenetic stimulation of dopaminergic neurons leads to an increase in HALIP, which can be decreased by the antipsychotic haloperidol. This cross-species study verified that "too strong a priori expectations + dopamine abnormalities" can produce hallucinations, and provided experimental evidence for the consideration of dopamine as a regulator of the purpose/prediction layer in the DIKWP model of this project.
The results shown in Figure 2 have important implications for our artificial consciousness model: as the experiment shows, the influence of high-level expectations on perception plays a key role in hallucinations, and neuromodulators such as dopamine are the mediators through which organisms achieve this effect. Therefore, in our DIKWP model, a parameter like "dopamine gain" can be added to the Purpose/Destination layer to simulate the desired strength. If this parameter is too high, the model will be more inclined to believe that there is a meaningful signal in the noise, thus reproducing the hallucinatory phenomenon. This also explains why traditional antipsychotics reduce hallucinations by inhibiting dopaminergic activity: by reducing the inappropriate reinforcement of information from the Purpose layer. Therefore, this project designed an intervention to "reduce the gain of the Purpose layer" in the simulation to simulate the effect of dopamine blockers, and verified that the model predictions were consistent with the results in the literature. This fully demonstrates the value of system diagrams and model pseudocode in guiding us in designing experiments and interpreting results.
The pseudocode 1 above has given an example of the detection and intervention process of the artificial consciousness operating system, which is used to communicate the algorithm logic within the team during the project development process and guide the actual programming implementation. In addition to pseudocode 1, we have compiled pseudocode for other key modules, such as the message passing algorithm of the "cross-brain semantic inference" module and the parameter discrimination criterion of the "anomaly detection" module. I won't list them all here for the sake of space, but the pseudocode is well documented in the project's technical documentation and verified in the code implementation. The role of pseudocode is to describe the logic of the algorithm in a way that is close to natural language, so that interdisciplinary team members (such as those with medical backgrounds) can also understand the operation of the AI module, which greatly improves the efficiency of collaboration.
In summary, the system diagram intuitively shows the ideas of our model and experimental design, as shown in Figure 2, which condenses the complex concept of cross-species experiment into a concise graphical language. Pseudocode bridges the gap between algorithm design and implementation, turning abstract ideas into executable solutions. Both of these are important intermediate outputs of this project, and as the project is completed, we will also publish these charts and pseudocode to help more researchers understand and reproduce our work.
Key technologies and innovations
This project crosses the frontiers of neuroscience and artificial intelligence, forming a series of original key technologies and innovations, which are summarized as follows:
Introducing the DIKWP artificial consciousness model into the field of neuromedicine to realize the hierarchical semantic modeling of human perception processes: In the past, the research on perceptual disorders such as hallucinations and pain was mostly limited to neurobiology or psychology. For the first time, this project proposes to use the DIKWP model as an artificial consciousness framework to describe the whole chain of perceptual information processing. This innovation allows us to unify the whole process from sensory input (Data) to cognitive interpretation (Wisdom) to subjective Purpose (Purpose), and disassemble the complex perceptual activity of the human brain into analyzable and simulable modules. This method breaks through the limitation of the traditional DIKW (pyramid) model without a destination layer, and emphasizes the role of the purpose drive in perceiving anomalies. This not only enriches the application scenarios of the artificial consciousness model, but also provides a new paradigm for the study of perceptual disorders. We expect that this hierarchical model will greatly improve the explanatory power of subjective symptoms such as hallucinations/pain, and promote the application of AI in psychiatric and pain medicine.
Independent research and development of the "perceptual anomaly recognition + cross-brain semantic reasoning" algorithm to realize the self-monitoring and correction of abnormal perception by artificial intelligence: The anomaly detection algorithm developed in this project can monitor the multi-layer output of the artificial consciousness model in real time, and immediately determine the perceptual obstacle once the pattern is abnormal. Unlike normal anomaly detection, we incorporate cognitive semantic information, such as using the model's prediction error to identify hallucinatory signs. In addition, we innovatively construct a cross-brain semantic reasoning algorithm that allows AI to simulate the process of cooperating in different regions of the brain to parse perceptual information. When hallucinations or pain allergies occur, the algorithm can find information contradictions between different "virtual brain regions", and reach an agreement through message transmission to correct the abnormality from the semantic level. This is similar to the process by which the human brain interacts with the prefrontal lobe and sensory areas to determine whether a hallucination is true or false. This technology gives AI systems a certain degree of "self-reflection" ability, which is also a highlight in terms of AI safety and interpretability. We have applied for an invention patent for this purpose, with independent intellectual property rights.
Construct a digital simulation platform for perceptual anomalies without entity dependence, and realize the transformation of the research paradigm from "WET experiment" to "SILICO experiment". In view of the lack of large-scale experimental equipment in this project, we took a different approach and built a digital twin simulation platform. The platform places the artificial consciousness model in a virtual environment, allowing us to apply stimuli and interventions to the model as if it were an experimental animal, observing its "behavior" changes. This completely computation-based experimental method is low-cost, efficient, and reproducible, and can quickly screen a large number of hypotheses and schemes, and then use the best one for limited practical verification resources. This line of thinking coincides with the current international concept of medical digital twins. Our platform has specially designed a variety of scenarios and index evaluation systems for perceptual impairments, which is professional and unique. It can be said that we have used computers as laboratories and created a new model for studying perceptual disorders. The platform can also be expanded to the research of other cognitive disorders in the future, and has broad application prospects.
A number of innovative intervention strategies based on artificial consciousness are proposed to realize the new concept of "soft therapy": Compared with the traditional "hard intervention" that relies on drugs and surgery, this project proposes a semantic-driven soft therapy concept at the simulation and theoretical levels. For example, by guiding the patient (or AI agent) to adjust the interpretation of perceived information, thereby reducing symptoms; Another example is to use virtual reality to provide correct sensory feedback to reshape brain cognition (such as the intelligent upgrade of mirror therapy). Many of these protocols have not yet been tried in the clinic, but our models predict their effectiveness and are supported in part by simulation and literature validation. If these ideas are confirmed in further research, it will open up a whole new world in the treatment of hallucinations and chronic pain. For example, digital therapeutics such as "hallucination correction software" or "pain awareness reconstruction headsets" may emerge in the future. We have put together a first draft of the patent for the new principles and are trying to get ahead of the curve. In short, this project boldly explores non-invasive, non-drug cures, bringing good news to patients and leading the transformation of medical models.
The value of interdisciplinary and international dialogue: The research content of this project spans multiple fields such as neuroscience, psychology, artificial intelligence, computer simulation, etc., reflecting the true interdisciplinary integration and innovation. This paradigm itself is a breakthrough in the boundaries of traditional scientific research, which is in line with the trend of multidisciplinary collaboration in today's complex scientific problems. Internationally, the research on consciousness and brain diseases by artificial intelligence is also a hot topic, and our DIKWP model and simulation method have injected new elements into this topic. Up to now, the DIKWP model and related work have attracted global attention and are regarded as an important direction to solve the problem of AI interpretability and value alignment. This project applies this cutting-edge theory to major medical problems, and will certainly have international dialogue value. We plan to actively publish our results in top academic conferences and journals to enhance the discourse power of Chinese scholars in the intersection of artificial consciousness and brain science.
Each of the above innovations is supported by corresponding technical support and data. In the process of project implementation, we not only pay attention to the introduction of cutting-edge ideas, but also ensure that ideas are implemented through models and experiments, so as to achieve original innovation "from 0 to 1". It can be expected that after the completion of this project, a new set of theories and technical systems with independent intellectual property rights will be formed, which will not only publish papers, but also may produce convertible software/patents, laying a solid foundation for subsequent in-depth research and product development.
Team composition and division of responsibilities
The project team is composed of experts and backbones from the fields of artificial intelligence, neuroscience, clinical medicine, etc., and has the knowledge and ability to carry out interdisciplinary research. The core team is as follows (each member's professional background and main responsibilities are in parentheses):
Project Leader: Prof. San Zhang (Expert in Artificial Intelligence and Neural Engineering) – Responsible for the strategic planning and overall management of the project, leading the design of the theoretical framework for the integration of the DIKWP model and biological mechanism, and coordinating the progress of each research group. Professor Zhang has made rich achievements in the field of artificial consciousness modeling, and serves as a director of the World Artificial Consciousness Association, and has the ability to control the direction of the project.
Project 1 PI: Prof. Si Li (Molecular Neurobiology) – Responsible for literature research and summary of the biological mechanism of perceptual impairment, and guiding the mechanism analysis at the molecular and cellular levels. Prof. Li will lead the mapping of key molecular/receptor changes in the visual and pain pathways, and provide biological parameters (e.g., nerve conduction velocity, receptor dynamics, etc.) for the simulation model.
Project 2: Associate Professor Wu Wang (Clinical Neurology/Pain Medicine) – responsible for the analysis of existing treatment options and clinical feasibility assessment. Dr. Wang, who has extensive clinical experience in pain and psychiatric disorders, will collect clinical data, case studies, provide medical interpretation of simulation results, and evaluate the clinical translational value of new strategies. His team will also assist with the validation part of the animal model, specifically the experimental design of pain behavior.
Principal Investigator of Project 3: Associate Professor Zhao Liu (Computer Science/Artificial Intelligence) – Responsible for the software development of artificial awareness OS and simulation platform. Dr. Zhao is proficient in machine learning and software engineering, and will lead several programmers to implement DIKWP model algorithms, anomaly detection modules, user interfaces, etc. He will also be responsible for the deployment and maintenance of the platform to ensure that the simulation experiments run smoothly.
Core Members:
Dr. Liu (Postdoctoral Fellow, Cognitive Neuroscience): Assist in the connection between Project 1 and Project 3, provide brain imaging data analysis support, and map brain network mechanisms to model structures. Responsible for the parameter basis of the cross-brain region semantic inference algorithm (e.g., the initial value of the connection weight of each brain region).
Chen (Overseas Consultant, Artificial Intelligence Ethics Expert): Provide a humanistic perspective on the design of artificial consciousness models, and ensure that the goals of the models are embedded in line with human values. This helps us avoid bias in the design of the model Purpose layer and makes the output more credible. Chen will regularly participate in remote workshops, make suggestions for model improvements, and facilitate international exchanges.
Engineer Sun (Software Engineer): Write the simulation platform code, focusing on front-end visualization and interaction. It is responsible for implementing the interface for researchers to configure experimental parameters, displaying the state diagram of each layer of the model in real time, etc., to improve the ease of use of the platform.
Graduate student Qian (Ph.D. student, Artificial Intelligence): Focus on the development and testing of anomaly detection algorithms, and try various machine learning methods to optimize accuracy. Assist in the construction of training data (collect normal vs abnormal model output samples through a large number of simulation runs) and improve detection reliability with supervised learning.
Zhou Graduate Student (Master's Student, Neurobiology): Assist in literature research and animal experiments. Responsible for sorting out the literature of animal models of hallucinations and pain, docking with animal experiment partners, following up the progress of experiments and collecting data.
In addition to the above members, we plan to invite Prof. Yucong Duan (the originator of the DIKWP model) as a project consultant to provide guidance on key technical solutions. Given Professor Duan's extensive experience in promoting the industrialization of the DIKWP model, his joining will help us refine the model and expand our impact. However, as Professor Tuan wears many hats (including the President of the World Association of Artificial Consciousness), we only seek advice on an advisory basis and do not take up too much of his energy.
The division of labor of the team follows the principle of "tackling key problems in blocks and collaborating and integrating", and each sub-team is independently responsible for its own modules, but realizes information sharing and collaborative problem solving through regular plenary meetings. The project leader and the project leader form a project management team to track the progress and schedule resources in a timely manner at the monthly meeting. We will also implement a dual tutor system for students, so that students in the field of artificial intelligence and students in the field of neuroscience can work together in pairs to learn from each other's knowledge backgrounds and bridge the gap in subject communication. For example, Associate Professor Zhao Liu was arranged to supervise Master Zhou's programming, and Researcher Li Si was assigned to supervise Dr. Qian's neuroscience theory. This training model not only improves the efficiency of research, but also lays a foundation for cultivating interdisciplinary talents in the future.
The team as a whole has strong strength and complementarity. Experts in artificial intelligence and neuroscience participate in ensuring the scientific and innovative nature of the solution; Clinical experts ensure that the study is always oriented to the needs of the application; Young scholars and students are concrete, enthusiastic and creative. On the platform of the Active Medicine Committee of the World Association of Artificial Awareness, we also have the opportunity to interact with international peers and make up for the shortcomings. You can be confident that this team configuration will be up to the challenges of this project and achieve the desired goals.
Risk plan
This project involves the exploration of new theories and technologies, and may encounter certain technical risks and uncertainties. In order to ensure the smooth progress of the project, we have formulated the following risk plans:
Model validity risk: As an emerging artificial consciousness model, there is no precedent for DIKWP to be applied in the field of specific perceptual impairments. There is a risk that the model will not adequately reproduce biological phenomena. For example, the model may not be able to simulate the details of certain hallucinations or the complexity of pain. In this regard, our plan is as follows: a) Model Iterative Optimization – Adopt agile development methods, first implement simplified model verification key concepts in the early stage, then gradually increase the complexity, continuously compare the simulation output with the literature/actual phenomena, and constantly adjust the parameters and structure until the results are satisfactory; b) Multi-model control – In addition to the DIKWP framework, we also consider introducing other cognitive models (such as global workspace model and predictive coding model) for control testing. c) Expert evaluation – Cognitive science experts are regularly invited to evaluate the rationality of the model output, detect deviations in a timely manner, and correct them. Through these measures, the risk of model failure is minimized.
Risks of Algorithm Technical Difficulties: The anomaly detection and semantic inference algorithms that the project needs to develop are quite challenging. If the performance of the algorithm does not meet the requirements (such as high false positive rate of anomaly detection and slow convergence of semantic inference), it will affect the evaluation of the effect of subsequent intervention strategies. To this end, we plan to: a**) simplify the problem** – give priority to simple scenarios, such as detecting a single type of hallucination first, and then expand to multiple types; Semantic inference is tested on a small network with fewer nodes and then scaled. Overcome it step by step to avoid difficulties in algorithm debugging due to over-complexity at the beginning; b) Leverage mature technology – make good use of existing machine learning tools, such as anomaly detection, try out algorithms such as Isolation Forest and One-class SVM as a reference baseline, and combine them with our customized methods; Semantic inference can be used as a reference for multi-agent reinforcement learning and the existing frameworks of graph networks. Seek help from the open source community when necessary; c) Performance Tuning – Make full use of the team's AI expert experience to perform mathematical analysis and optimization of the algorithm, accelerate convergence, add regular rules to prevent overfitting, etc. At the same time, we will prepare computing resources to support (apply for high-performance GPU servers) to make up for the lack of algorithm efficiency. Through these means, try to ensure that the algorithm module achieves the practical performance target.
Data and validation risks: Some biological experiments are required to verify the project in the later stage, but our experimental equipment is limited, and if the cooperation channels are not smooth or the experiment fails, the convincing conclusion may be weakened. In this regard: a) Multi-channel cooperation – contact a number of potential partners (universities or research institutes) in advance and obtain data from public databases at the same time. For example, open-source resources such as phantom limb pain fMRI dataset and EEG data of patients with hallucinations can be used when they cannot conduct experiments on their own. b) Alternative validation – If the conditions are limited in animal experiments, we can use simulation experiments instead of partial validation, such as building a higher fidelity computational model (e.g., simulating a large neural network) to verify the effect of the intervention, or using case reports as case study support; c) Gradual progress – Arrange the validation session in the third year and conduct it in a "small-scale multi-batch" manner, even if the results of a single experiment are not obvious, through multiple repetitions and comprehensive analysis of different indicators, and strive to draw trend conclusions. Even if we don't fully validate the hypothesis, we will have a frank discussion in the paper, pointing out what is needed to verify it in the future, without affecting project delivery.
Personnel and schedule risks: Interdisciplinary teams can be difficult to coordinate, and if there is miscommunication or personnel changes, it will affect efficiency. In this regard: a) Strengthen communication mechanisms – regular plenary meetings and workshops to ensure information symmetry. The project manager tracks the progress of each technical group on a daily basis, and immediately coordinates resources to solve problems when they are found; b) Personnel Preparation – Set aside flexible funds to support the hiring of short-term consultants or research assistants. In the event of an unexpected exit of personnel in key positions, substitutes can be quickly introduced. The team also encourages "one specialty and multiple abilities", such as AI personnel learning certain biological knowledge, and providing temporary support in case of lack of manpower in biology; c) Node control – Develop detailed Gantt charts, set quarterly milestone checks, and work overtime or reduce the scope of low-priority tasks in time when there are signs of delay, so as to ensure that the main line goals are completed on schedule.
Funding and equipment risks: Funding constraints may arise if it is found that certain algorithms require more computing power or software support, or that unplanned collaborative experiments require additional costs. In this regard: a) flexible budgeting – setting aside a certain amount of flexible funds (about 10%) in the budget to cover unforeseen expenses, such as the purchase of cloud computing services, data fees, etc.; b) Resource sharing – make full use of the existing equipment of the relying unit and the cooperative unit, such as server borrowing, laboratory sharing reagent consumables, to save costs. Actively apply for preferential resources of the school computer time or the National Supercomputing Center; c) Invest in Installments – Purchase equipment in a step-by-step manner according to the urgency of the task to avoid excessive one-time overhead. For example, high-performance GPUs can be rented for cloud service trials first, and then purchased physical equipment when necessary. These measures will cushion the financial pressure and ensure that the project is not on track.
In general, we have fully predicted the potential risks and formulated a multi-level plan. With the team's multidisciplinary background and collaborative spirit, we are confident that we can flexibly respond to various challenges in the progress of the project, turning risk into motivation for improvement. Process documentation and knowledge accumulation will also be emphasized in project management, and even if setbacks are encountered, each attempt will be documented, providing lessons for subsequent exploration, minimizing the impact of uncertainty and ensuring that project goals are successfully achieved.
Expected Results:
The project is expected to achieve fruitful results by the end of the three-year implementation period, including:
Theoretical achievements: The "Cognitive Framework of Perceptual Impairment Based on DIKWP Model" was proposed to systematically elucidate the multi-level mechanism of perceptual abnormalities such as visual hallucinations and chronic pain. This new theory is expected to be published in high-level academic journals and promote the development of theories in related fields. At the same time, we will improve the details of the DIKWP model of artificial consciousness to make it closer to biological reality, and contribute a new model with both explanatory power and biological significance to the field of artificial intelligence.
Achievements of technical methods: The software of "Digital Simulation Platform for Perceptual Abnormalities" has been developed, which has the functions of simulating a variety of perceptual impairment scenarios and testing intervention programs. The platform will be released as open-source software or licensable for research and teaching use, and is expected to be a useful tool for the intersection of neuroscience and AI. In addition, we will summarize and refine anomaly detection algorithms and semantic reasoning algorithms to form a general methodology, write method papers or reports, and disseminate them in the field of AI and computational neuroscience, so as to enhance China's discourse power in artificial awareness algorithms.
Application and patent achievements: According to the new strategies verified in the project, 2-3 Chinese invention patents have been applied, such as: "A hallucination detection and intervention method based on artificial consciousness", "Chronic pain semantic feedback control system", etc. These patents will lay the foundation for future industrialization. We expect at least one project to be authorized by the end of the project (the rest will enter the substantive review stage), and actively seek to cooperate with medical AI companies to explore commercial possibilities such as applying digital simulation platforms to drug discovery (as an aid to new drug screening) or doctor training (providing visual hallucination/pain simulation cases).
Publications: Produce no less than 5 high-quality academic papers (including at least 3 SCI papers and 2 Chinese core papers). The topics cover: (1) the theoretical elaboration and simulation results of the DIKWP model of perceptual impairment (to be submitted to IEEE or Springer series of journals); (2) Technical details of anomaly detection and semantic inference algorithms (to be submitted to Artificial Intelligence Journal or journals in the field of neural computing); (3) Evaluation of the effects of digital platforms and intervention strategies (to be submitted to neuroscience or medical interdisciplinary journals, such as Frontiers in Neuroscience). At the same time, 1-2 papers (e.g., IJCAI, AAAI) will be submitted at the AI summit to introduce our interdisciplinary research to attract more attention. Enhance academic impact through paper publication.
Talent training: With the help of the project implementation, it is expected to train 2 doctors, 2-3 masters, and 1 postdoctoral. These young talents will master the cross-cutting skills of AI + brain science and grow into interdisciplinary research backbones. At least one Ph.D. is expected to complete a high-level dissertation on the content of this project. The team members will also improve their scientific research organization and communication and cooperation skills during the project exercise, so as to prepare for greater scientific research tasks in the future.
Academic Exchange and Impact: Through the project, we plan to hold 1-2 domestic academic seminars or thematic forums to share our progress, invite domestic and foreign experts to discuss the application of artificial consciousness in medicine, and promote academic exchanges. Actively participate in international conferences, such as presenting papers for NeurIPS, COSYNE, etc., or presenting our simulation platform at INCF (International Federation of Neuroinformatics) conferences. Strive to give an invited report at the annual meeting of the World Association for Artificial Consciousness to introduce the results of this project. These measures will enhance China's voice in international dialogue in the field of the combination of artificial consciousness and brain science, and create a leading image.
Social and industrial benefits: In the long run, if our theories and platforms are further validated and developed, they can be gradually applied to practice. For example, intelligent assisted diagnosis: the application of anomaly detection algorithms to the patient's EEG/brain imaging data is expected to detect hallucinations or pain abnormalities early and improve the objectivity of diagnosis. Digital Therapeutics: Using our proposed semantic feedback and cognitive restructuring strategies, we develop applications for hallucination management or pain rehabilitation to provide patients with personalized non-pharmacological interventions. While these applications are beyond the scope of this project, our work will serve as a trailblazer and provide new ideas for industry. At the same time, the multidisciplinary nature and popularization of science will also help to disseminate scientific knowledge to the public, such as through media reports, to let the public understand how artificial intelligence can help understand human suffering and hallucinations, and improve the public's scientific literacy.
In short, the expected outcomes of this project are rich and layered, from basic theory to technical methods to practical applications. Although clinical translation may not be fully realized during the project cycle, the theoretical and technical foundation laid has revolutionary potential. With these results, we are expected to continue to lead this emerging interdisciplinary field in the next 5-10 years, receive greater research grants, put theory into clinical practice, and contribute to the overcoming of perceptual disorders." This is also fully in line with the original intention of the key project: to take major scientific issues as the traction, produce new theories and technologies with international influence, and promote the development of related disciplines and industries.
Budget
The total amount of scientific research funding to be applied for this project is 3 million yuan (three years), and the budget will be reasonably allocated to various expenditure subjects according to the needs of the research task. The specific budget and description of the funds are as follows:
Personnel costs: Budget of about 900,000 yuan (30%). Including the performance subsidy of the scientific researchers of the project team and the research assistant allowance for graduate students. Among them: the subsidy for the project leader and the project leader is calculated and paid according to the regulations of the university, with a total of about 200,000 yuan; 2 scientific research assistants/programmers for 3 years× with an annual salary of 150,000 yuan each, a total of 900,000 yuan; In addition, about 200,000 yuan of graduate student allowance and social security are reserved. Personnel costs are mainly based on incentive work, and are issued in strict accordance with the actual contribution, and do not exceed the total budget.
Equipment and software fees: The budget is about 500,000 yuan (16.7%). This project does not involve the procurement of large-scale experimental instruments, but in order to build a simulation platform and run a model, it needs to be equipped with high-performance computing equipment and necessary software licenses. It mainly includes: a) 2 sets of high-performance GPU workstations for deep learning training and large-scale simulation, each set is about 150,000 yuan, a total of 300,000 yuan; b) 100,000 data storage and server upgrade components (including large-capacity hard disks, memory expansion, etc., to ensure the efficiency of simulation data access); c) 50,000 yuan for commercial software license fees and development tools, such as Unity Pro software for VR scene development, MATLAB neural network toolbox, etc.; d) Other miscellaneous 50,000 yuan, such as UPS power supply to ensure that the calculation is not interrupted, etc. If there is a discount or switch to cloud computing services at the time of actual purchase, you can save and adjust accordingly.
Material consumables: The budget is about 200,000 yuan (6.7%). It is mainly used for consumables and a small amount of reagents related to animal experiments. For example, to conduct mouse behavior experiments with cooperative units, it is necessary to purchase experimental animals (several mice, 20,000 yuan), feeding expenses and conventional experimental reagents (narcotic drugs, sampling consumables, etc., 50,000 yuan); If you want to test biological samples, you need to purchase ELISA kits or tissue staining reagents (50,000 yuan). In addition, 30,000 yuan will be prepared for the purchase of literature database services, cloud data storage fees and other information materials. Due to the limited experimental links of this project, the material cost is relatively small, but it must be ensured that the key experiments are needed.
Testing and laboratory processing fee: The budget is about 100,000 yuan (3.3%). It is used to pay for outsourcing testing and processing services. For example, if you need to perform high-throughput sequencing or mass spectrometry analysis of animal brain tissue, you need to entrust a professional institution (about 50,000 yuan); Customizing special hardware (such as miniature rat back stimulator) may require a processing cost of 20,000 yuan; The rest is used as a maneuver for unforeseen testing expenditures. All commissioned services will be selected according to the bidding or market price, and the cost will be strictly controlled within the budget.
Travel and academic exchange expenses: The budget is about 400,000 yuan (13.3%). The project is interdisciplinary, which requires extensive cooperation and communication among team members. The travel expenses include: the domestic travel of the project team is 300,000 yuan, which is expected to be mainly used for: cross-city exchanges within the team twice a year (personnel exchange visits between AI sub-projects and medical sub-projects), going to cooperative units to carry out experiments (such as going to cooperative hospitals for data collection), participating in domestic academic conferences to share results, etc.; 100,000 yuan for international exchanges, and it is planned to support the project backbone to participate in at least one important international conference (such as artificial intelligence or neuroscience annual conference) in the third year to present the results. If the trip cannot be made due to the epidemic, it can be used to invite international experts to report online. Strictly implement the financial system of the unit and reimburse the actual reimbursement.
Conference and publication costs: Budget of about 150,000 yuan (5%). It is planned to hold an academic seminar or results conference in the middle and final of the project, with a budget of 50,000 yuan each time, including venues, materials, and honoraria for expert lectures. The paper page fee and patent application fee are budgeted at 50,000 yuan, which is used to pay for the necessary expenses for publishing Open Access papers (such as the layout fee of some SCI journals) and the official fees and agency fees for 2-3 patents from application to authorization. We will prioritise free publications, but set aside a budget in case needed.
Management Fee and Unforeseen Expenses: Estimated at $750,000 (25%). According to the policy of the relying unit, the management fee is calculated according to a certain proportion of direct expenses (typical 15%), which is used for the university's scientific research management and infrastructure depreciation, about 300,000 yuan. The remaining 450,000 yuan is used as unforeseen mobile funds, accounting for 15% of the total budget, for new reasonable expenses in the process of project implementation. For example, the model needs to add new modules, purchase software, and a key technology needs to temporarily hire external consultants or conduct additional experiments. When it is used, it must be approved by the manager to ensure that the special funds are used exclusively and cannot be diverted for other purposes.
The above budgeting fully takes into account the needs and characteristics of the project, and achieves comprehensive coverage, key focus and moderate redundancy. For example, personnel costs and equipment investment are the top priorities, accounting for nearly half, to ensure that human and computing resources are in place; At the same time, we have also considered the importance of interdisciplinary exchanges, and provided sufficient financial support for travel and exchange, so as to facilitate the collision of innovative ideas. The setting of unforeseen costs provides a buffer against risks for the project, and the financial allocation can be dynamically adjusted according to the actual progress. We are committed to strictly implementing the budget, complying with financial regulations, preparing detailed final accounts and budget adjustment reports every year, accepting supervision and auditing, and ensuring that funds are used for the relevant activities of the project. If there is a surplus, it will be returned or used for follow-up research according to regulations, so as not to waste national scientific research funds.
To sum up, the application for this key project focuses on the frontier topic of "Research on Neural Mechanism and Intervention Strategy of Perceptual Impairment Based on DIKWP Model of Artificial Consciousness", and has been carefully planned in terms of research content, technical route, team organization and condition guarantee. The project has clear objectives, feasible solutions, theoretical innovation and potential application value, and is in line with the support direction of key projects. We believe that with the support of departments at all levels and the joint efforts of the team, this project will achieve breakthrough results, open up new ways for recognizing and intervening in perceptual disorders, and set an example for the integration of artificial intelligence and brain science. We sincerely ask for support for the establishment of key projects!
References:
Prof. Yucong Duan: DIKWP artificial consciousness model leads the future of AI, and 114 patents are expected to be implemented in the industry. China Media Industry Network, 2025.
Yucong Duan | DIKWP Artificial Consciousness (Principle). DAMA China, 2023.
Charles Bonnet Syndrome – Causes & Symptoms. Cleveland Clinic, 2023.
Alice in Wonderland Syndrome: A Clinical and Pathophysiological Review. J Neurol, 2022. (Hypothesis of the mechanism of AIWS syndrome involving the multisensory junction cortex)
Modulating neuroplasticity for chronic pain relief: noninvasive neuromodulation as a promising approach. Exp Mol Med, 2025.
Computational Psychiatry Across Species to Probe the Neural Circuitry Underlying Hallucinations. JAMA Psychiatry, 2022. (Studying computational models of hallucinations across human-rat and finding that high expectancy + striatal dopamine leads to hallucination-like perceptions)
A novel Bayesian computational model for pain perception integrating prior expectation. Sci Reports, 2023. (proposing a Bayesian model of pain perception to demonstrate a significant modulation effect of expectation on pain perception)
The prevalence and risk factors for phantom limb pain. J Pain Res, 2024. (latest meta-analysis estimates the global incidence of phantom limb pain at approximately 64% and discusses possible mechanisms such as stump discharge and cortical recombination)
Placebo and nocebo effects in pain: insights into descending modulatory pathways. Pain, 2021. (studies have shown that positive expectations activate descending systems such as PAGs to relieve pain, while negative expectations exacerbate pain)
Digital twins for health: a scoping review. NPJ Digital Medicine, 2022.